Tissue Typing for Allogeneic Transplantation

Allogeneic stem cell transplantation involves the use of stem cells from someone other than the patient. The donated stem cells can come from either a person related or not related to the patient.
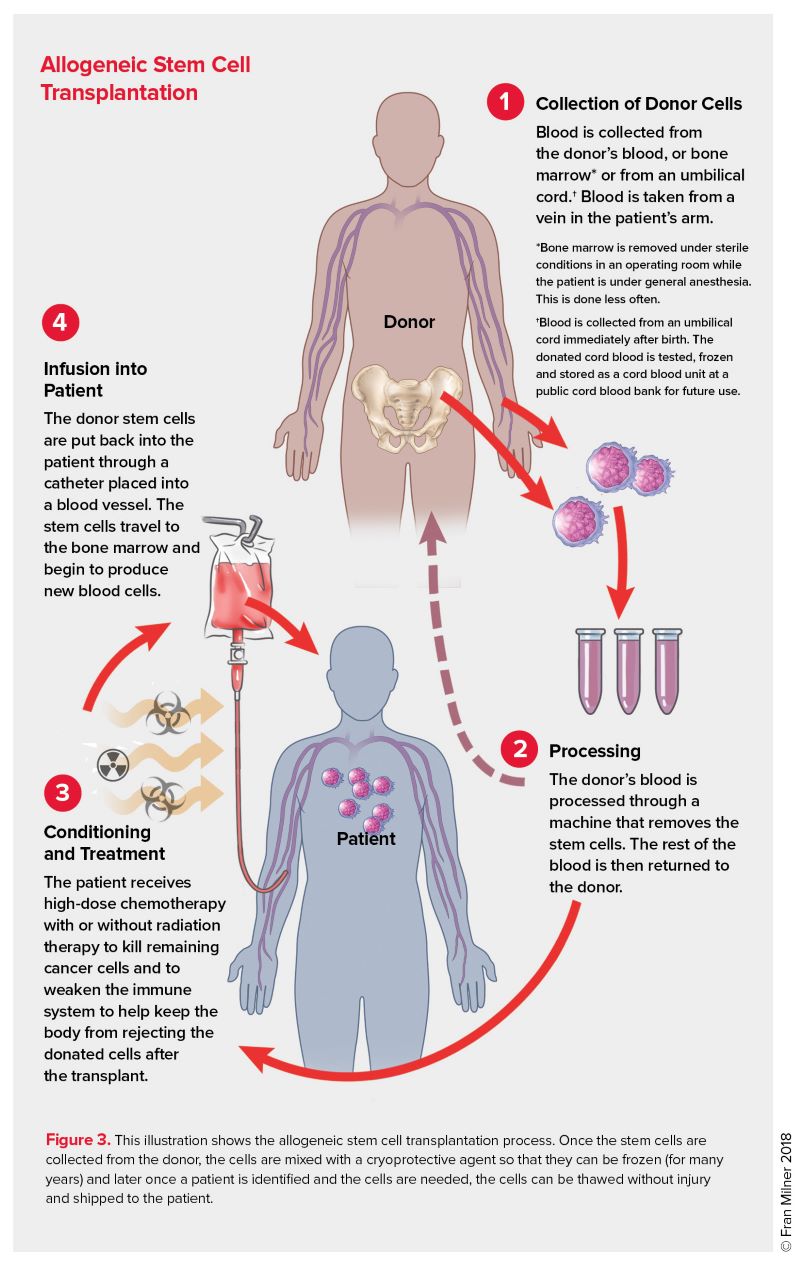
Before beginning an allogenic SCT, the patient receives a conditioning treatment that consists of either chemotherapy or radiation. Some patients receive both. Conditioning treatment is given to destroy any remaining cancer cells in the body. It weakens the patient's own immune system so that the donor cells are not rejected. Conditioning treatment allows the new cells to move through the bloodstream to the patient's bone marrow, where the donor cells begin to grow and produce new blood cells, including red blood cells, white blood cells, and platelets. This process is called “engraftment.”
For some types of blood cancers, an allogeneic SCT may work directly to destroy cancer cells. This is called the graft-versus-tumor (GVT) effect. The GVT effect happens when white blood cells from the donor (the “graft”) identify any remaining cancer cells (the “tumor”) in the patient as foreign and attack them. For some patients, GVT is crucial for the effectiveness of their treatment. It can help prevent their cancer from coming back. This benefit can only occur in allogeneic SCT. It does not occur in an autologous SCT.
Allogeneic SCT is often used to treat blood cancers such as leukemia, myelodysplastic syndromes and myeloproliferative neoplasms.
Once it is determined that allogeneic SCT is a treatment option for a patient, the patient’s doctor will begin to search for a suitable donor. For most patients, a close match is important because it improves the chances for a successful transplant by:
HLA Matching. People have different sets of proteins or markers called human leukocyte antigens (HLAs) on the surface of most of their cells. They make up a person’s tissue type, which varies from person to person. Blood tests of both the patient and potential donor are done to determine if there is an HLA match.
There are many HLA markers. Individuals inherit half of their HLA markers from their mothers and half from their fathers, so most often the ideal donor is a patient’s sibling (who has inherited the same HLA markers). On average, a person has one chance in four of having the same HLA type as his or her sibling, but many patients do not have a sibling with the same tissue type. For those patients who do not have a matched family donor, an unrelated donor may be found through a volunteer donor registry.
Mismatched Unrelated Donor Transplantation. Your doctor will try to match 10 to 12 HLA markers to lower the risk of graft-versus-host disease (see below). In recent years, advances in medicine have allowed for the use of stem cell donors who are mismatched, meaning that not all 10 or 12 markers are a perfect match. Use of medications following transplant allow for mismatched donors while still lowering the risk of graft-versus-host disease.
Haploidentical Transplantation. To increase the number of potential donors, some transplant centers have begun to perform half-match (haploidentical) transplants for patients who cannot find a closely matched
HLA donor. In many cases, a healthy first-degree relative (a parent, sibling or child) can be a half-match donor and donate stem cells. Because a child receives half of their HLA markers from a parent, a biological child and their parent will always be a half match, while there is only a 50 percent chance of a sibling being a half match. As a result, most individuals will have a suitable related haploidentical donor.
Cord Blood Transplantation. Cord blood is blood taken from the umbilical cords of newborn babies. Cord blood may be an option for patients without a well-matched donor. Unfortunately, cord blood units tend to contain fewer stem cells and may be difficult to use in people with larger body sizes. Cord blood transplant patients also have an increased risk of graft failure. However, cord blood is available much more quickly (potentially within 2 to 4 weeks), while it may take a month or more to obtain matched unrelated donor grafts. Another advantage of cord blood transplants is that cord blood may require a lower level of HLA matching between the donor and recipient.
One complication of allogeneic transplantation is that the patient’s body—despite the treatment to suppress the immune system—may reject the donated stem cells before they are able to engraft in the bone marrow. The patient’s immune cells may see the donor’s cells as foreign and destroy them.
Graft-versus-host disease (GVHD) is a common but potentially serious complication of standard allogeneic and reduced-intensity allogeneic SCT. Sometimes, the cells from the donor (graft) sense that healthy cells of the patient (host) are foreign and attack and damage the patient’s normal cells. GVHD can be mild, moderate or severe. In some cases, it can be life-threatening.
A close HLA match between the donor and patient helps to lower the risk of GVHD. There are also medications that help prevent GVHD. Even with a close HLA match and medication, some people still get GVHD.
Allogeneic stem cell transplants for patients who are older or have overall poor health are relatively uncommon. This is because the pre-transplant conditioning therapy is generally not well tolerated by such patients, especially those with poorly functioning internal organs. However, reduced intensity allogeneic stem cell transplants may be an appropriate treatment option for certain patients who are older, who have diseases that involve major organs, such as the heart or liver, or who are otherwise not healthy or strong enough to undergo standard allogeneic transplantation.